06/09/2021
Acupuncture and Moxibustion in Japan
日 本 鍼 灸


The Japan Society of Acupuncture and Moxibustion (JSAM)
公益社団法人 全日本鍼灸学会,東京
Cover page: Fugaku Sanjurokkei (Thirty-six view of Mt. Fuji), A woodblock print by Hokusai KATSUSHIKA (葛飾北斎1760-1849)
Foreword
To establish academic acupuncture and moxibustion (Acumoxology)
The Japan Society of Acupuncture and Moxibustion (JSAM) was established in 1980 by reorganizing the Japan Society of Medical Acupuncture and Moxibustion (JSMA) and the Japan Acupuncture and Moxibustion Society (JAMS) into one academic society. Last year marked the 40th anniversary of our founding. The purpose of its establishment was to become the center of “academic acupuncture and moxibustion (acumoxology) ” in Japan and contribute to their development.
Just as there are “clinical medicine”, “basic medicine”, and “social medicine” in the field of medicine, I consider that “acumoxology” includes “clinical acupuncture and moxibustion”, “basic acupuncture and moxibustion”, and “social acupuncture and moxibustion”. Since acupuncture and moxibustion were originally therapeutic sciences, there have been many reports on clinical acupuncture and moxibustion such as case reports and case series, but research on basic acupuncture and moxibustion is not as active as previously. In addition, social acupuncture and moxibustion must be developed further in the near future. Since the JSAM is an academic organization, it has a mission to provide members with a place to present their research results and promote their research. In addition, it is necessary to educate undergraduate students in these three fields. “Acumoxology” cannot be established only by therapeutic science, and I consider that future development cannot be expected without basic and social acupuncture and moxibustion.
Japanese acupuncture and moxibustion, like those in the world, originated in ancient China and were introduced via the Korean peninsula about 1,500 years ago, but they have evolved in a way that is very different from modern Chinese or Korean medicine. To preserve this tradition of Japanese acupuncture and moxibustion, and further develop them, we would like to pursue the necessary projects and proceed with them one by one.
August 2021
Ikuro Wakayama, MD. PhD.
President
The Japan Society of Acupuncture and Moxibustion (JSAM)
Ⅰ.History of Acupuncture and Moxibustion in Japan
1. Early history of acupuncture and moxibustion in Japan
[B.C.]
Archeological evidence has revealed that in ancient times, stone-gimlets, stone-needles, bone-needles, etc., were used in medical treatment for the same purposes as acupuncture needles today.
[6th Century]
Due to improved transportation and communication with the Asian Continent, Chinese medicine was introduced to Japan together with Buddhism and came to be used as a form of religious medicine. Medicine of ancient Japanese origin gradually lost its popularity.
[8th Century]
The Taiho Ritsuryo (大宝律令: Taiho Code) was enacted in 701 A.D., revising the Japanese medical system and defining the status of professors, doctors, students, etc.
[10th Century]
Japan’s first medical text, the Ishinpo (医心方), was written by Yasuyori TAMBA (丹波康頼, 912-995). The contents of this book were based on Chinese medical texts compiled during the Sui (隋) and Tang (唐) dynasties.
[12th Century]
Many textbooks on acupuncture and moxibustion started to be published in Japan in this era, although most of the descriptions were quoted from Chinese literature.
[16th Century]
Due to the influence of Dosan MANASE (曲直瀬道三, 1507-1594), Buddhist ethics, which had until this time played an important role in medical philosophy, were replaced by Confucianism. It was from this time that Japanese acupuncture and moxibustion began to develop in directions independent of China.
[17th Century]
Oriental medicine derived from ancient China has went unique developments in Japan, and the style of Traditional Japanese Medicine has been established. Up until 17th Century, needles had been made of iron, but thereafter, silver and gold needles came into use in Japan. During this era, “needling with hammer” method (Figure 1) was developed, and Isai MISONO (御薗意斎, 1557-1616) disseminated it to many practitioners. Guide tube (Figure 2), a small cylindrical tube through which the needle is inserted, was also developed in this era for the first time in the world. This “needling using guide tube” method enabled practitioners quite simple and speedy needle insertion. Waichi SUGIYAMA (杉山和一, 1610-1694) disseminated this method, and it is used today in Japan by over 90% of acupuncturists, and globally by many practitioners.

Figure1. Hammer and Needl 
Figure 2. Needle (40 mm, φ0.16 mm) and Guide tube
Traditional Japanese Medicine was very popular during this era, and various schools of thought on the subject began to appear. Roughly, the schools could be divided into two groups, the theoretical group, which based its practices on ancient Oriental medical teachings, and the practical group, which regarded the practical clinic as very important.
[18th Century]
One of the unique acupuncture methods developed in this era was infant acupuncture therapy. Using spatula-like or rod-like needles (Figure 3), acupuncturists stimulated the infant’s skin by fine touching or rubbing (non-penetrating needle method). Infant acupuncture therapy became popular in the Kansai area, the western part of Japan, particularly in Osaka, and the target condition of infants was short-temperedness or crying at night.
During this era, Japanese acupuncture and moxibustion were spread to Europe by the Portuguese Jesuit Luís Fróis (1532-1597) for the first time, but more precise information was introduced to Europe by the Dutch medical doctor Willem ten Rhijne (1647-1700) and German medical doctor Engelbert Kaempfer (1651-1716): both came to Japan at the end of the 17th Century. Later, Kaempfer wrote “The History of Japan (日本誌 )” in 1727, in which he described Japanese acupuncture and moxibustion along with other unique aspects of Japanese culture. It is notable that he used the word “moxa” for the first time in the world in this book, derived from the Japanese word “mogusa (burning grass)”.

Fig. 3 Spatula-like and rod-like non-penetrating needles for infants
[19th Century]
Dutch and German medicines were introduced and became popular in Japan. A new system of medicine was established; however, acupuncture and moxibustion, considered types of folk medicine, were not included within the realm of this medical system. Thus, Oriental medicine did not prosper during this era.
2. First half of the 20th Century
People had another look at the efficacy of acupuncture and moxibustion, and these became a professional field. Research and experimentation were conducted in the manner of Western medicine. Kinnosuke MIURA (三浦謹之助, 1864-1950) discovered that acupuncture-moxibustion therapy improved blood circulation. Research concerning the conformity between acupuncture meridian points and Head’s zones was conducted during this period. Influenced by Western medical practices, acupuncture-moxibustion experiments and research were conducted on animals. The existence of meridians was ignored in the treatment of individual diseases, as diagnoses by Western medical methods became popular, and treatment was practiced by acupuncturists.
Some of the major discoveries regarding the mechanisms of acupuncture and moxibustion made during this period were: increase in leukocyte and erythrocyte counts; increase in the number of complements and antibodies; alkalosis changes in bone and blood; intensification of intestinal peristalsis; and acceleration of liver functions.
Pharmacological studies indicated that the results mentioned above occurred as a result of the histotoxin formed when moxibustion was administered. Hidezurumaru ISHIKAWA (石川日出鶴丸, 1878-1947) reported that experiments on animals proved that the acupuncture-moxibustion mechanism was effected through the autonomic nervous system. On the other hand, interest in the meridians was revived, and Sorei YANAGIYA (柳谷素霊, 1906-1959) and his colleagues developed the “meridian therapy”.
3. Acupuncture and moxibustion in Japan in the 1940s, after the Second World War
In 1945, when Japan was occupied by the Allied Forces, Douglas McArthur’s General Headquarters (GHQ) ordered the Japanese Government to ban acupuncture and moxibustion as a barbarous and unscientific therapy. This was due to the fact that some Japanese soldiers used acupuncture or moxibustion on Allied Forces prisoners of war (POWs), with utterly good intentions because of the medical supply shortage, but the POWs took it as a form of torture, and some of those Japanese soldiers were subsequently indicted as war criminals.
That was a period of real crisis for acupuncture and moxibustion. First of all, a number of acupuncturist guilds got together and started to launch a big campaign against the decree. Also, some scientists in Western medicine who were interested in the scientific aspect of the therapy, particularly ISHIKAWA and Takeshi ITAKURA (板倉武, 1888-1958) took the lead in this movement. They were successfully able to prove certain scientific facts regarding the efficacy of acupuncture and moxibustion. Thanks to those enthusiastic movements, McArthur’s GHQ rescinded the ominous order.
Under the guidance of the GHQ, democratization, modernization, and scientification in every social aspect became the number one priority. In order to cope with such demands, acupuncture guilds started to enhance both the educational level of new students and the qualitative level of those already licensed. And for the purpose of scientification, the “Institute of Oriental Therapy” was established in 1945, financially supported by the guilds and headed by the then most prominent scientists in the field — ISHIKAWA and Kyugo SASAGAWA (笹川久吾, 1894-1968).
4. Characteristic clinical features of current acupuncture and moxibustion in Japan
Currently, acupuncture and moxibustion are making a significant contribution to the health of Japanese people, and practitioners are upholding the 1,500-year-old tradition.
There are many unique diagnostic and treatment methods that were developed in Japan. Typical examples are shown in Fig. 4 to 8. They are the guide tube insertion method (Fig.4), direct moxibustion using “refined moxa floss” (Fig.5), infantile non-penetrating acupuncture (Fig.6), intradermal needle acupuncture (Fig.7), and Pyonex press tack needle treatment (Fig. 8a, 8b)

Fig.4 Guide tube insertion method 
Fig.5 Non-scarring direct moxibustion

Fig.6 Infantile non-penetrating
acupuncture method
Fig.7 Intradermal needle method

Fig.8a Pyonex press tack needle (0.6mm) 
Fig. 8b Pyonex press tack needle pasted on the skin
Ⅱ.The Japan Society of Acupuncture and Moxibustion
1. JSMA and JAMS during the 1940s–1970s
Thence forward, many institutes or scientific groups have assembled and disassembled, and by around 1950, two groups became the most outstanding in size and quality: Nihon Shinkyu Igaku Kai (日本鍼灸医学会, Japan Society of Medical Acupuncture: JSMA) established in 1948, and the Nihon Shinkyu Chiryo Gakkai (日本鍼灸治療学会, Japan Acupuncture and Moxibustion Society: JAMS), established in 1951. JSMA, chaired by Kyugo SASAGAWA of Kyoto University, had as its main objective scientific research on the mechanism of acupuncture and moxibustion. Places of its activity were medical universities in western Japan, i.e., Kyoto, Osaka, Nagoya, etc., and its members consisted mainly of medical doctors, medical students, and some acupuncturists.
JAMS, chaired by Etsunosuke HIGUCHI (樋口鉞之助), dealt with scientific research on the therapeutical art of acupuncture and moxibustion. Places of its activities were medical universities and acupuncture colleges in eastern Japan, i.e., Tokyo, Tohoku etc., and members consisted mainly of acupuncturists, acupuncture students, and some medical doctors and students.
In 1977, when the two societies cooperated in organizing the Fifth World Conference of Acupuncture of SIA (Société Internationale d’Acupuncture, with its head office in Paris), staff members of both societies realized that it would be more beneficial to merge the two societies for the development of acupuncture-moxibustion science. The Ministry of Health and Welfare (MHW, later MHLW: Ministry of Health, Labour and Welfare) of Japan also felt that the two should be merged for the better administration and control of NGO researchers.
2. JSA (then JSAM) during the 1980s–2000s
Thus, in 1980, the two societies merged into a new society, and the Zen Nihon Shinkyu Gakkai (全日本鍼灸学会, Japan Society of Acupuncture: JSA) was established, with Kentaro TAKAGI (高木健太郎, 1910-1990), dean of the Nagoya City University as President and Hideo YAMAMURA (山村秀夫, 1920-2017), professor of the University of Tokyo, as Vice-President. JSA’s objective is to enhance the progress of the art and science of acupuncture-moxibustion through activities on research, education, and academic exchange nationally, as well as internationally. Since 1999, the Society’s English name has been changed to the Japan Society of Acupuncture and Moxibustion (JSAM).
Today, JSAM actively works on the annual scientific meeting, with the different regional divisions taking turns in hosting it. Many local small and medium-size lecture/study meetings, and national and international exchanges of scientific news are also the important activities of the society. It encourages and subsidizes scientific activities of educational institutions and any other activity deemed to meet its objective. Its quarterly publication, the Zen Nippon Shinkyu Gakkai Zasshi (全日本鍼灸学会雑誌, Journal of the Japan Society of Acupuncture and Moxibustion: JJSAM) is distributed to its members, and online English Journal, The Japanese Acupuncture and Moxibustion (JAM) is open to free access.
JSAM has provided services to WHO for the development of acupuncture-moxibustion science. JSAM as a principal member of 1st Committee of Meridian Points of Japan (1965-69, 1973-1989), played a key role in the development of the WHO Standard Acupuncture Nomenclature for 1981-1989 (“Standard Acupuncture Nomenclature” in 1984 with the following editions including those with eight different language codes; WHO Regional Office for the Western Pacific (WPRO), Manila, the Philippines) by contribution of Kiichiro TSUTANI (津谷喜一郎, WPRO Medical Officer) under the guide of Hiroshi NAKAJIMA (中嶋 宏1928-2013, WPRO Regional Director). Those pamphlets and books were widely distributed in the world. Thereafter, its second edition was published in 1993.
During the first meeting of the Working Group on Standardization of Acupuncture Nomenclature in Manila in 1982, Yukio KUROSU (黒須幸男) proposed the establishment of the World Federation of Acupuncture-Moxibustion Societies (WFAS), which was finally established in 1987 in Beijing after much debate and discussion. JSAM hosted the WFAS Third World Conference on Acupuncture (WCA’93) in Kyoto in 1993 with more than 3,000 participants from 38 countries and area. During WCA’93, the Workshop on Clinical Research Methodology on Acupuncture was held. It paved the way for the organization of the WHO Working Group on Clinical Research Methodology, which met in Aomori, Japan, in 1994 and developed “Guidelines for Clinical Research on Acupuncture” (WHO Regional Publication, Western Pacific Series No.15, 1995). The guidelines served as a springboard for the development of evidence-based acupuncture. In 2016, JSAM hosted WFAS International Symposium (WFAS Tokyo/Tsukuba 2016) with more than 1,700 participants from 31 countries and area.
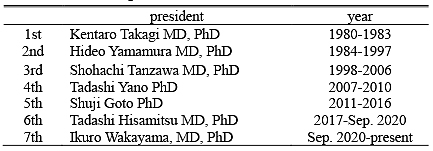
The present number of registered members of JSAM in March 2020 is 3,741, composed of medical doctors, dental doctors, researchers, acupuncture-moxibustionists, and undergraduate/postgraduate students. The Executive Board of JSAM consists of 20 Directors, among whom one President and two Vice-Presidents are elected. The Board of Counselors has 48 elected members from all branches. Successive presidents of the JSAM are listed in Table 1. In 2021, Ikuro WAKAYAMA(若山育郎) is serving as the president of the society.
Table 1. Successive presidents of the JSAM
3. Increasing academic exchange with the East Asian and Western countries
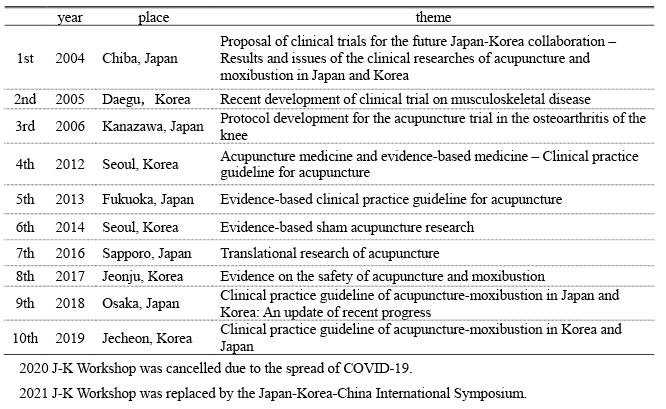
To facilitate the academic exchange of scientific acupuncture research in the East Asia, JSAM signed an agreement with Korean Acupuncture and Moxibustion Society (KAMS, later The Korean Acupuncture and Moxibustion Medicine Society; KAMMS) and Korean Oriental Medicine Society (KOMS, later The Society of Korean Medicine; SKOM) on 14 February, 2004. According to this agreement, JSAM formally started collaborating in a research program, “Japan-Korea Workshop on Acupuncture and EBM”, with KAMS in Chiba in 2004. An actual preparatory meeting was held at Takamatsu in 2003. Since then, series of the “Japan-Korea Workshop on Acupuncture and EBM” has been hosted alternately by JSAM and KAMMS. Table 2 shows the past workshops.
In addition, JSAM hosted the series of International Symposium on Acupuncture. First was held on osteoarthritis of the knee in 2006 in Kyoto. The 2nd was on low back pain in 2009 in Saitama, and the 3rd was on headache in 2012 in Yokkaichi, Mie. JSAM invited domestic and international highly reputable speakers in each field from Germany, Spain, the United Kingdom, Sweden, Switzerland, the United States, Canada, China and Korea, and the symposium ended very successfully. JSAM held Japan-Korea-China International Symposium virtually in 2021 due to the spread of Corona Virus Disease-19 (COVID-19). The main theme of this symposium was ICD-11 and ICHI.
Table 2. A chronological table of the Japan-Korea Workshop on Acupuncture and EBM
4. JSAM and the standardization of the Traditional Medicine – WHO and ISO
In 2002, Seung-hoon CHOI from Korea became a fourth medical officer for the Traditional Medicine of the WHO/WPRO. He started four projects regarding the standardization of traditional medicine. In 2003, CHOI began a project to standardize the point locations of meridian points. Accordingly, we organized the 2nd Committee of Meridian Points of Japan (2004-2012, chaired by Shuichi KATAI), consisting of 5 acupuncture-related societies or organizations in Japan, to join the project. Altogether 15 meetings were held, and the outcome was published in 2008 as a book, entitled: “WHO Standard Acupuncture Point Locations in Western Pacific Region”. It has been highly recommended by acupuncture practitioners in East Asia as well as in the Western countries.
Besides locations of meridian points, Choi put other projects on the table for discussion, i.e., terminology, information, and clinical practice guidelines (CPGs) of traditional medicine. The outcome of the project of standardizing terminology was published in 2008 as a book, entitled: “International Standard Terminology of Traditional Medicine in Western Pacific Region”.
Japanese delegates who participated in the series of meetings were invited personally by WPRO, independent of any Japanese academic societies or associations, which caused certain problems in the sound development of the project. Thus, the Japan Liaison of Oriental Medicine (JLOM), consisting of major societies of traditional medicine in Japan was established in 2005. Presently, manufacturers of traditional medicine in Japan that provide Kampo medicinal drug, acupuncture-moxibustion device, and other medical equipment related to traditional medicine have joined JLOM. In addition, JLOM is receiving support from Japanese Government. JSAM plays an important role in JLOM in the fields of acupuncture and moxibustion.
Since 2010, JSAM is continuing to send delegates to meetings of ICD (International Classification of Disease) and ISO (International Organization for Standardization) as mentioned below.
The project incorporating the classification of traditional medicine into ICD was discussed as a part of the “standardization of information” project, and it was one of the projects that CHOI launched in 2003. Although the project was not completed because he left WPRO in 2008, it was approved by the WHO HQ as a part of the revision of the ICD-10 project in 2009 through active lobbying. Thus, the first WHO Meeting on International Classification of Traditional Medicine was held in Hong Kong in May 2010. The series of meetings was held and experts including China, Japan, and Korea discussed the issues for more than 8 years. JSAM along with the Japanese Traditional Acupuncture and Moxibustion Society (JTAMS) dispatched experts to the meetings, and proposed the development of a classification system with their descriptions of meridians and collateral patterns which was incorporated into ICD-11. The draft classification of traditional medicine was released on 18 June, 2018 as “Traditional medicine conditions Module 1” in Chapter 26 of ICD-11. We carried out field tests using meridians and collateral Patterns of 2,620 patients in acupuncture and moxibustion clinics in Japan. The Traditional Medicine Chapter was finally approved on 28 May 2019 as supplementary chapter (Chapter 26) at the 72nd session of the World Health Assembly (WHA).
While WHO/WPRO publishes the outcomes of international standardization of traditional medicine, Standardization Administration of China (SAC) proposed ISO to establish a Technical Committee (TC) to develop standards for Traditional Chinese Medicine. The proposal was approved by a vote by National member bodies and TC249 was set up in ISO in September 2009. In the preparatory meeting of TC held in August 2009, delegates from China, Japan, Korea, and Australia discussed and agreed to put the highest priority on setting an International Standard (IS) for the quality and safety of medicinal products and medical equipment over other items.
The 1st plenary meeting of TC249 was held in Beijing in June 2010, just one week after the International Classification of Traditional Medicine (ICTM) meeting of WHO. So far, ISO has held 11 plenary meetings of TC249 (The 11th plenary meeting was held virtually on June 1st-29th, 2021 due to the spread of COVID-19). IS of traditional medicine are being developed in 6 working groups. Among them, working groups developing the standards of acupuncture and moxibustion are as follows.
WG3: Quality of acupuncture needles and safe use of acupuncture
WG4: Safety and quality of medical devices other than acupuncture needles
WG5: Terminology and informatics
JWG1: ISO/TC 215 WG: Informatics
ISO/TC249 has published seventy ISO standards as of 1 August 2021, and Japan played a leading role in establishing an intradermal needle standard (ISO 18746:2016 Traditional Chinese medicine – Sterile intradermal acupuncture needles for single use) and test method standard for acupuncture needle for electrical stimulation (ISO 20487:2019 Traditional Chinese medicine -Test method of single-use acupuncture needles for electrical stimulation). In addition, Japan is serving as a project leader to set 3 standards for diagnostic equipment involving an electroacupuncture stimulator and tongue diagnosis (ISO 20498 Computerized tongue image analysis system — Part 2: Light environment, Part 3: Color chart, Part 4: Peripheral visual instruments) in WG 4.
ISO/TC215, with its mission to establish standards for health informatics, is dealing with informatics of traditional medicine in Traditional Medicine Task Force (TMTF) under WG3 of TC215. In TC215, Japan led a project to develop IS for acupuncture point informatics (16843-1:2016 Health informatics – Categorical structures for representation of acupuncture — Part 1: Acupuncture points), and the standard was published as Technical Specification in 2016.
Presently, ISO/TC249 is actively working on many proposals, and JSAM, as a member made up of Japanese delegates, is making every effort and playing an important role in contributing to the development of necessary IS in the fields of acupuncture and moxibustion in the world.
Ⅲ.Current Status of Licensing and Education for Acupuncturists in Japan
1. Licensing system
Only licensed physicians, licensed acupuncturists, and licensed moxibustionists may provide acupuncture and moxibustion treatment in Japan. The license of an acupuncturist or moxibustionist is specific to that person and to that field of practice. (あん摩マツサージ指圧師、はり師、きゆう師等に関する法律Legislation No. 217, Article 1, 12 December 1947)
2. Licensing requirements
Applicants must have graduated from an acupuncture and moxibustion school recognized by the Ministry for Health, Labor, and Welfare (MHLW) of Japan or from a university (or in the case of the visually impaired, from a school for the blind or a center for the visually impaired) recognized by the Ministry of Education, Culture, Sports, Science, and Technology (MEXT). These graduates must also pass a national examination by the MHLW.
3. Current status of the national examination
Local qualifying examination had been conducted by each prefectural government until 1991, but presently the national examination is given under the auspices of the MHLW, and is administered by the Foundation for Training and Licensing Examination in Amma Massage-Acupressure, Acupuncture, and Moxibustion (http://www.ahaki.or.jp/).The first national examination was given in 1993, and examinations have been offered annually since then. The examination, which is given at 50 locations throughout Japan, consists of 180 multiple-choice questions. A score of 60 is required to pass.
The national examination does not include any practicum testing, which is left to the discretion of each school. A number of provisions are made to increase the fairness of this examination for visually impaired applicants, who are permitted the use of Braille and sound recordings, and who are allowed extra time to complete the examination (1.5 times longer than for sighted students). The ratio of sighted to visually impaired examinees is approximately 9:1.
Topics for the acupuncturist examination (general medical treatment, sanitation, public health, related legislation, anatomy, physiology, general pathology, introduction to clinical medicine, particulars of clinical medicine, rehabilitation medicine, general theory of Oriental medicine, general theory of the meridians and acupuncture points, clinical theory in Oriental medicine, acupuncture theory).
Topics for the moxibustionist examination (general medical treatment, sanitation, public health, related legislation, anatomy, physiology, general pathology, introduction to clinical medicine, particulars of clinical medicine, rehabilitation medicine, general theory of Oriental medicine, general theory of the meridians and acupuncture points, clinical theory in Oriental medicine, moxibustion theory).
From 2020, new topics such as kinesiology, pathophysiology, social security system and professional ethics were added in both examinations.
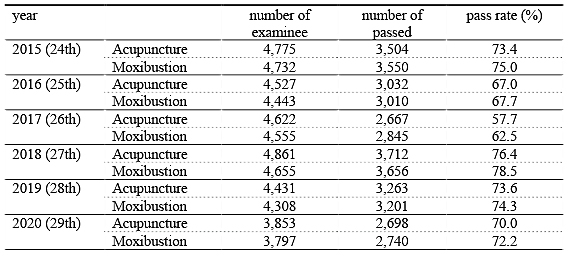
Recent pass rates are shown below (Table 3). License for acupuncturist and that for moxibustionist are independent in Japan, but almost 98 % of them have both licenses. Therefore, “鍼灸師, acupuncture-moxibustionist” that means acupuncture-moxibustion practitioner is commonly used in Japan.
Table 3. Recent pass rates of national examination
4. Current status of education
As of August 2021, there are 10 universities and 81 acupuncture schools for the sighted in Japan, of which 46 (2 universities and 44 private vocational schools) were members of the Japan College Association of Oriental Medicine. In 1999 there were only 28 schools throughout Japan, but this number has increased since the legislation regarding acupuncture-moxibustion education had been reformed in 2000.
There are 69 schools in Japan for the visually impaired (1 university and 68 publicly funded schools for the blind or centers for the visually impaired), with approximately 300 students. These schools except university offer a 3-year program in preparation for the acupuncturist/moxibustionist examination, with the option of also studying simultaneously for the examination for Amma massage/shiatsu massage therapist. Students also have the option of enrolling in the program preparing for the Amma massage/shiatsu massage therapist national examination only.
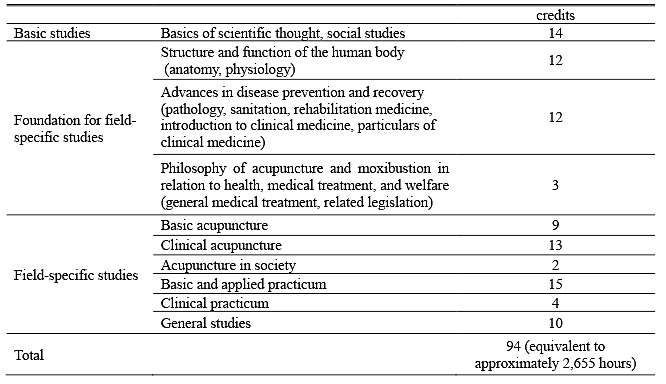
Required courses and credits (hours) in the 3-year-course acupuncture school is shown in Table 4. Credits are calculated on the basis of specifications established for Japanese universities (1 lecture credit = 15 to 30 hours, 1 seminar credit = 15 to 30 hours, 1 practicum credit = 30-45 hours, 1 clinical training = 45 hours).
In 2004, the credit system was introduced and the former lists of categories and detailed descriptions of course contents were eliminated. In addition, clinical practicum became mandatory in 2018. These changes were made in order to produce high-quality practitioners to meet the citizen’s trust and expectations.
The Japan College Association of Oriental Medicine (JCAOM https://www.toyoryoho.or.jp/) and Japan Association of Massage & Acupuncture Teachers (JAMAT http://www.rikyouren.com/) are working together to develop educational guidelines, publish standard textbooks, standardize educational content, and maintain high standards of quality.
Table 4. Courses and credits in 3-year-course acupuncture school
5. Current status of graduates
Five surveys on the status of graduates of schools were performed every five years by the JCAOM in 1996, 2001, 2006, 2011, and 2016.
1) The male-female ratio of graduates in 2016 (n=2,615) was 1.03. The ratio was decreased when compared to that in 1996 (1.98, n=2,601), indicating that the number of female graduates has been increased. The most common age range for male was 30 to 34, and that for female was 21 to 24 in 2016.
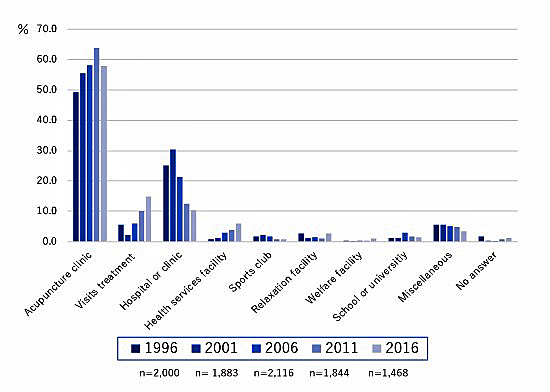
2) The 2016 survey showed 76.2% of graduates practicing professionally. The percentage decreased when compared to that in 1996 (84.2%). A higher percentage of male graduates (78.3%) were in professional practice than their female counterparts (75.0%) in 2016, but the difference was getting smaller compared to those in 2001 (87.3% and 80.4%, respectively). Graduates not in professional practice accounted for 18.0% of the total, up slightly from the 1996 survey (15.1%). A major change was noted in working circumstances. Considerably more graduates were running their own practice in 2016 (34.5%) than in 1996 (21.3%). The rest of graduates are practicing acupuncture as employees. Graduates who were employed by a clinic or hospital accounted for 30.4% of the total in 2001, but down significantly to 10.4 in 2016. Instead, graduates worked in acupuncture-related treatment clinics or judo-orthopedist clinic, facilities for visit treatment, and health service facilities were increased (Figure 4).
3) Conditions of patients who came for acupuncture treatments of 1996, 2001, 2006, 2011 and 2016 are shown in Figure 5. Low back pain was the most common complaint, followed by shoulder stiffness, knee joint problems, leg pain, shoulder joint problems, cervicobrachial syndrome, indefinite complaints, general health maintenance, sports injuries, headache, and gynecological conditions. There was little change among five surveys except for the decrease in cervicobrachial syndrome and increase in indefinite complaints, headache and gynecological conditions.
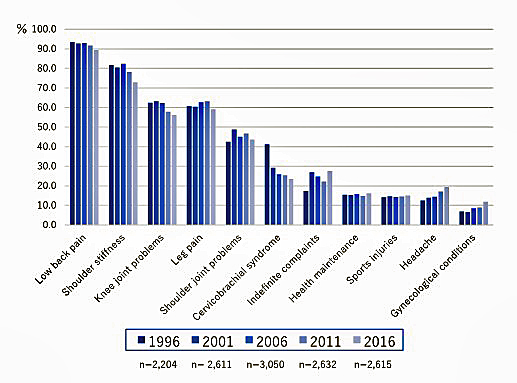
(Surveyee selected five most common conditions)
6. Number of licensed practitioners and number in actual practice
After passing the national examination, acupuncturists must register with the MHLW in order to apply for a license. As of April 2019, the MHLW rolls showed 176,386 registered acupuncturists and 175,270 registered moxibustionists in Japan. However, in fact, not all of them are working. A survey by the MHLW in 2018 indicates that there are approximately 120,000 acupuncture-moxibustionists working in Japan today.
7. Acupuncture and National Health Insurance System in Japan
In Japan, acupuncture and moxibustion are covered by National Health Insurance in six disease conditions, only when a patient with these diseases was not improved using conventional Western medical treatments and when there is a written consent from a medical doctor. Those are six diseases, i.e., neuralgia, rheumatoid arthritis, cervicobrachial syndrome, frozen shoulder (scapulohumeral periarthritis), low back pain, and cervical spine sprain sequelae (whiplash injury). Total cost of acupuncture and moxibustion treatments covered by National Health Insurance accounts for USD 360 million (JPY 40 billion) per year. [One USD in August 2021 was approximately 110 JPY.]
In most acupuncture and moxibustion clinics, however, acupuncture and moxibustion are not covered by health insurance, and are considered as discretionary treatments. The cost varies markedly by region and practitioner, but is generally in the range of USD 27 (JPY 3,000) to USD 64 (JPY 6,000) per session. The market is considered to be approximately USD 822 to 914 million (JPY 90 to 100 billion).
The original version of this text was drafted by Mr. Masayuki YOSHIKAWA (吉川正行), vice Director, Department of International Affairs, JSAM, in 1995. Ver. 2: revised on 1 November 1999 by Dr. Kiichiro TSUTANI (津谷喜一郎), Director, Department of International Affairs, JSAM, Mr. Takeshi KITAGAWA (北川毅), and Mr. Kazuhiko HORIGUCHI (堀口和彦), members, Department of International Affairs, JSAM. Ver. 3: revised by Dr. TSUTANI and Mr. HORIGUCHI on 1 November 2000, with merging the text of “The development of acupuncture and moxibustion in Japan” written by Mr. Yukio KUROSU (黒須幸男) of the Japan Acupuncture and Moxibustion Society (JAMS) in 1975. Ver.4: relation with WHO was included on 10 October 2002. Ver. 4.4: revised on 5 Mar.ch, 2006. Ver.4.5: revised on 20 October 2006 by Dr. Hiroshi TSUKAYAMA (津嘉山 洋), member Department of International Affairs, JSAM and Dr. Ikuro WAKAYAMA (若山育郎), Director, Department of International Affairs, JSAM. Ver.5: the new chapter regarding the licensing and education system was added by Dr. Shuji GOTO (後藤修司), Vice President of JSAM in September 2007. Part of the new chapter was reprinted from The Journal of Kampo, Acupuncture and Integrative Medicine (KAIM) .2006; 1 (Special edition): 12-13, with permission from the executive editor of the Journal. Ver.6: the new chapter regarding “JSAM and the standardization of the Traditional Medicine – WHO and ISO” was added by Dr. Toshihiro TOGO (東郷俊宏), a former secretary general of the Japan Liaison of Oriental Medicine (JLOM). Ver.7: the chapters “JSAM and the standardization of the Traditional Medicine – WHO and ISO”, “current status of education” and “current status of graduates” were amended by Dr. Toshihiro TOGO, an advisor of JLOM and the members of the Department of International Affairs of JSAM in 2021.

The Japan Society of Acupuncture and Moxibustion (JSAM)
公益社団法人 全日本鍼灸学会
Gakuen Bldg. 10F, Yoyogi, Shibuya-ku, Tokyo 151-0053, Japan
tel: +81-3-6276-6751, fax: +81-3-6276-6752, e-mail: honbu@jsam.jp, http://www.jsam.jp/
ver. 7.0 23 August 2021